COVID-19 Emergency Situation Report 5 (14 – 20 April 2020)
Highlights
- First fatality from COVID-19 recorded in East Jerusalem.
- First new COVID-19 cases in Gaza reported in nearly two weeks.
- The Inter-Agency Response Plan for the COVID-19 crisis is currently under revision to include emerging needs.
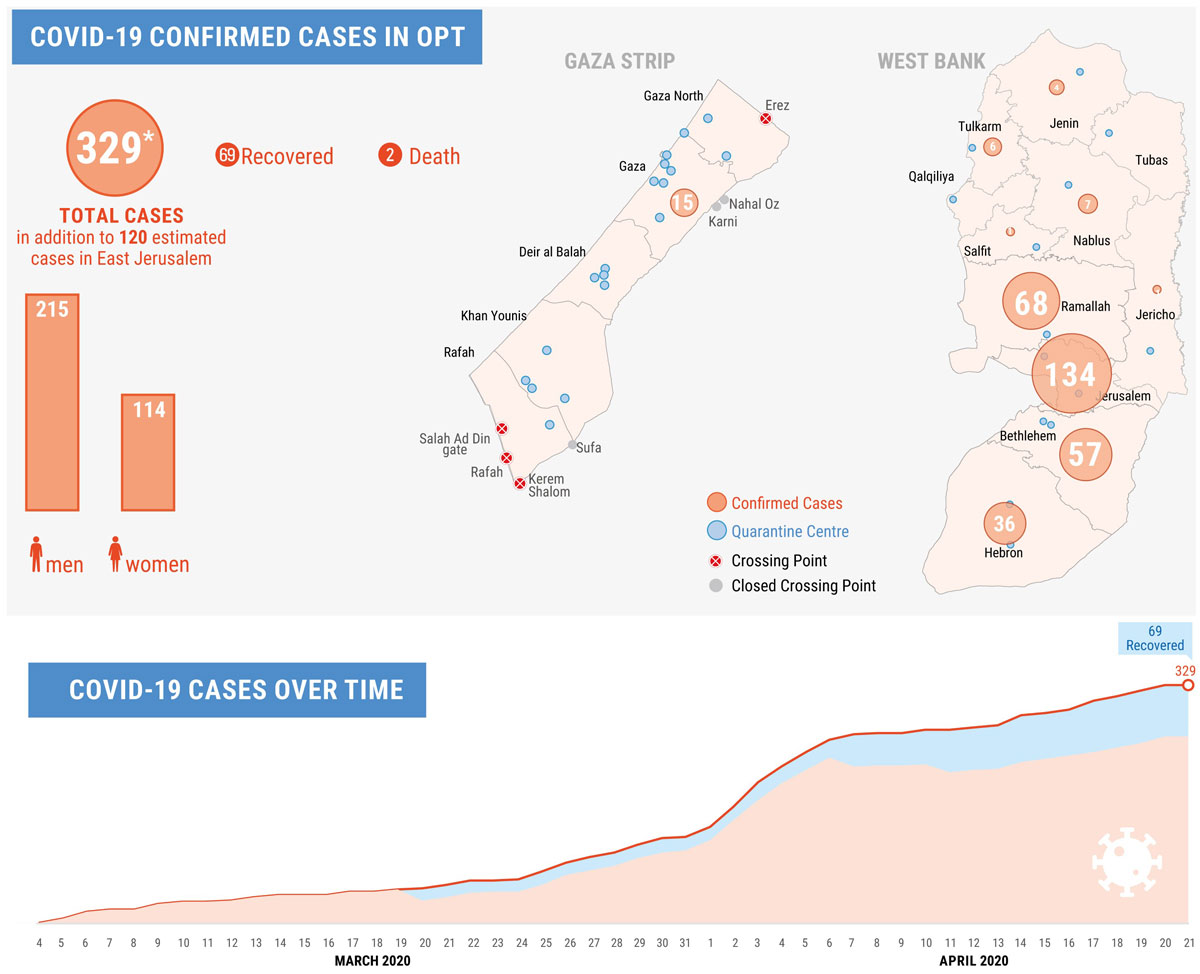
| 329 | 22,800 | 65 | US$34 M |
| People with COVID-19 (confirmed cases, exc. East Jerusalem) | Samples tested for COVID-19 | Quarantine and treatment centres | request for Inter-Agency Response Plan |
Situation Overview
As of 21 April, a total of 329 Palestinians are confirmed to have contracted COVID-19 in the OPT, excluding East Jerusalem: 314 in the West Bank, and 15 in the Gaza Strip. Two people have died and 69 have recovered. A total of 22,800 samples have been processed, according to the Palestinian Ministry of Health (MoH).
The first fatality in East Jerusalem, a 78-year-old woman from Al Issawiya, was recorded on 18 April: according to reports, still unconfirmed, a second woman died of the virus in Hadassah Hospital on the night of 20 April. The Palestinian MoH reported that as of 20 April, 120 Palestinians in East Jerusalem were detected positive. According to WHO, the situation in East Jerusalem regarding COVID-19 is being managed by the Israeli authorities and patients treated by the East Jerusalem Hospital Network (EJHN) and by Israeli hospitals.
Late on 20 April, Palestinian Prime Minister, Dr. Mohammad Shtayyeh, announced a series of relaxations to the State of Emergency that has been in force across the OPT since 5 March. While maintaining some movement restrictions and physical distancing, these relaxation measures are aimed to “ensure the gradual acceleration of the economic wheel in productive projects.” No date was given for the start of the relaxations, which could also be reverted, if “the spread of the virus is detected.”
In governorates with little or no infection recorded, including the Gaza Strip, “economic establishments that employ less than three workers, including agriculture, food, building workshops, garages, and individual professions, are allowed to work from 10 am to 5 pm,” while other establishments can open on Friday and Saturdays. In the more affected governorates, including Ramallah and Bethlehem, certain enterprises may open on “Sunday, Tuesday, and Thursday, with no more than three people in each workplace.” All governorates will remain isolated from one another, “except for the movement of trade, agricultural and food commodities, and medicines.”
Mosques, churches and other public places will remain closed and celebrations, including Ramadan gatherings are prohibited. Places of education will also remain closed, but the final school exam, the Tawjihi, will take place on 30 May. There will also be a partial resumption of banks, insurance and the stock market.
Asserting that the majority of Palestinians who contracted COVID-19 are labourers in Israel or people who were exposed to them, “the movement of workers between their workplaces inside Israel and their homes is prohibited until further notice.” Working in settlements is also strictly prohibited.
West Bank
Movement and social distancing measures remain in place, although certain relaxations appear imminent according to the latest announcement of the Palestinian Prime Minister, see above. Currently, 15,000 people are in quarantine centres across the West Bank, including in sixteen official and fourteen unofficial centres and medical facilities. A recent review conducted by a range of partners [1] has identified gaps in urgently needed medical equipment and supplies, including PPE, in the centres, as well as shortages in sanitation and hygiene materials for those in home quarantine. The Palestinian MoH has opened up new testing sites, including in Jenin and Hebron, in addition to the three existing centres, allowing for more extensive and rapid testing.
Six testing centres have been opened in East Jerusalem by the Israeli authorities. As of 20 April, the Palestinian MoH has reported 120 COVID-19 cases in East Jerusalem, including approximately 50 cases in Silwan. Al-Makassed and St. Joseph hospitals have been designated for COVID-19 management, with the other EJHN hospitals providing support. Three COVID-19 patients are currently treated in these hospitals; a number of medical staff, all West Bank ID holders, who have been in contact with these patients, have contracted the virus. WHO is coordinating with the network to address the most pressing needs, as the hospitals continue to suffer from chronic underfunding: a contribution of 9.5 million Euros has been received from the European Union to help address urgent funding requirements.
Thousands of Palestinian workers remained in Israel over the recent Jewish Passover holiday, as the Israeli authorities maintained the validity of their work permits. However, concerns have been raised again about their return, and the related risk of a spread of the virus, during the month of Ramadan, with a big influx expected at the beginning of the holiday later this week. Those who have returned have been registered by the Palestinian authorities and supplied with health information materials and instructions for home quarantine, although reaching unauthorized workers has been challenging as they avoid the official crossings, despite the efforts of the authorities and emergency committees to monitor their return.
Although the Allenby Crossing with Jordan remains closed, some 160 Palestinians who were quarantined in Dead Sea resorts were allowed to return to the West Bank last week, following their testing by the Palestinian authorities.
Since the beginning of the crisis, the Israeli authorities have largely frozen the demolition of inhabited homes but have continued targeting livelihood and service-related structures, adding strain to already vulnerable communities. The latter also stopped since the start of the Passover holiday (8 April) until 20 April, when two structures were demolished in the Nablus area. Search and arrest operations by Israeli security forces across the West Bank have also continued at a reduced frequency, significantly reducing tensions and clashes with residents. The surge in attacks by Israeli settlers in certain areas has continued, including multiple incidents of physical assault, arson and agricultural vandalism, with the number of incidents resulting in Palestinian injuries or property damage increasing by 80 per cent since the start of the crisis, compared to January-February. Israeli Security Force operations in Al Issawiya in East Jerusalem have also continued in the past weeks, although fewer incidents and clashes were reported.
Gaza Strip
For the first time since 6 April, two new cases were reported on 19 April, among a group of Palestinians who had returned to Gaza from Egypt last week. The two were quarantined immediately after their arrival in Gaza and transferred to the Rafah Field Hospital following their test result. This brings to 15 the number of positive cases in Gaza, of whom nine have recovered. As of 20 April, 3,338 samples have been tested for COVID-19 in Gaza, including some conducted in the West Bank and in Israel due to lack of capacity. The health authorities in Gaza continue to appeal for more support to procure additional testing kits. WHO reports, that while only 250 individual testing kits are currently available in Gaza, they will provide another 10 kits with a capacity to perform up to 2,000 individual tests on 22 April.
Over 2,000 people are currently staying in 21 active designated quarantine centres, including health facilities, schools and hotels, up from around 600 last week. This surge is due to the arrival of over 1,630 people, who returned to Gaza from Egypt between 13 - 16 April through the Rafah Crossing. All these arrivals have been quarantined in designated facilities for 21 days. Current procedures mandate testing on the fourth day of their quarantine, with a re-examination conducted on the twentieth day, just before the end of the mandatory quarantine period. In the absence of sufficient testing kits, the mandatory quarantine may be extended to 28 days.
Following its exceptional opening last week for the return of Palestinians from Egypt, the Rafah crossing is again closed, and the authorities have announced that they do not plan to open it again before 5 May, except for special cases. Some 2,000 Palestinians from Gaza currently in Egypt, have registered through an online platform and have still to return.
Despite the low number of confirmed COVID-19 cases in Gaza, WHO is encouraging people to adhere to the recommended measures, including physical distancing and personal hygiene measures. In cooperation with UNICEF, WHO continues efforts to procure essential ICU and ventilator equipment through global supply mechanisms.
The Israeli-controlled Erez crossing has been largely shut down since 12 March for the exit of most permit holders, except emergency cases and cancer patients. The return of Palestinians to Gaza via Erez has been allowed, with 51 entries recorded during the reporting period, all of whom have been placed in the mandatory 21-day quarantine.
The movement of goods from Israel and Egypt has continued as previously, including the entry of restricted (“dual use”) items via the Israeli-controlled Kerem Shalom Crossing. The Government of Israel has offered to expedite approvals for items needed in relation to the COVID-19 response.
Inter-Agency Response Plan – Funding Status
During the reporting period, around US$ 1 million additional contributions and pledges for COVID-19 humanitarian interventions were made, bringing the total to over $ 29 million. Thanks to more detailed information from donors and recipient organizations, it has been possible to disaggregate this amount by the specific interventions being funded, and distinguish between those included in the Inter-Agency Response Plan and others outside it.
Switzerland and South Korea increased their contributions to the OPT Humanitarian Fund to sustain local efforts in response to COVID-19. Their efforts, jointly with previous contributions from Belgium, Germany Ireland, Norway and Sweden, allowed the HC to rapidly scale up the response to support the Inter-Agency COVID-19 Response Plan through the fund.
Total funding for COVID-19 response by cluster (in Million US$)

COVID-19 response funding in the OPT (through and outside the Inter-Agency Response Plan)
| Cluster | Response Plan (RP) Requirements | Through the Response Plan | % of the RP covered |
Outside the Response Plan |
Total in US$ |
| Education | 1,132,000 |
660,000 |
58% | 1,735,000 | 2,395,000 |
| Food Security | 4,300,000 | 0% | 1,721,500 | 1,721,500 | |
| Health | 19,468,481 | 8,485,500 | 44% | 10,207,583 | 18,693,083 |
| Protection | 550,000 | 373,000 | 68% | 373,000 | |
| Shelter & NFI | 3,440,000 | 650,000 | 19% | 2,798,500 | 3,448,500 |
| WASH | 5,114,864 | 1,886,035 | 37% | 865,000 | 2,751,035 |
| Total | 34,005,345 | 12,054,535 | 35% | 17,327,583 | 29,382,118 |
Total Funding for COVID-19 Response by Donors
| Donor | Outside the Response Plan | Through the Response Plan | Total in US$ |
| Canada | 1,760,000* | 1,760,000* | |
| CERF | 300,000 | 300,000 | |
| DFID | 1,120,000 | 1,120,000 | |
| ECHO | 7,655,000** | 105,000 | 7,760,000** |
| Education Cannot Wait | 1,550,000 | 555,000 | 2,105,000 |
| Ireland | 138,000 | 138,000 | |
| Italy (IADC) | 35,000 | 35,000 | |
| Kuwait | 6,116,500 |
2,883,500 |
9,000,000 |
| NCA HQ, DCA | 71,035 | 71,035 | |
| Norway | 61,083 | 61,083 | |
| OPT Humanitarian Fund | 6,175,000 | 6,175,000 | |
| Oxfam | 60,000 | 60,000 | |
| UNESCO | 150,000 | 150,000 | |
| UNICEF | 627,000 | 627,000 | |
| WHO | 20,000 | 20,000 | |
| Grand Total | 17,327,583 | 12,054,535 | 29,382,118 |
* Commitments
** Attribution to the Inter-Agency COVID-19 Response Plane under verification.
Health Supplies Needs as per PA Revised Plan
| Item | Baseline West Bank | Delivered West Bank | Baseline Gaza | Delivered Gaza | Under procurement (overseas) | Total Needed (as per PA revised plan) | Gap |
| Testing items for no. ppl | 18,390 | 3,400 | 2,772 | 3,500 | 500,000 | (471,938) | |
| PCR machines | 1 | 1 | 6 | (5) | |||
| Patient monitor | 14 | 1,500 | (1,486) | ||||
| PPEs | 50,000 | 13,600 | 100,000 | (36,400) | |||
| Face masks | 13,800 | 6,550 | 165,000 | (144,650) | |||
| Ventilators | 175 | 120 | 100 | 1,200 | (905) | ||
| Oxygen concentrators | 15 | 150 | (150) | ||||
| ICU beds (PA) | 255 | 120 | 1,200 | (825) | |||
| ICU beds with ventilator (WHO sitrep) | 213 | 87 | 37 | 1,200 | (900) | ||
| Goggles/eye wear | 800 | 800 | 20,000 | (18,400) |
Coordination
The Inter-Agency COVID-19 Task Force led by the Humanitarian/Resident Coordinator (HC/RC), as well as the Inter-Cluster Coordination Group (ICCG), continue meeting regularly to follow up on the implementation of the InterAgency Response Plan. The HC/RC also informs the Palestinian authorities about essential movements required by humanitarian and development staff during this period of enhanced movement restrictions. Where necessary, coordination with the Israeli authorities is also conducted to ensure the safe movement of staff.
As part of the Inter-Agency Response Plan, UNICEF and WHO, with the support of the HCT’s Advocacy Working Group and UN Communications Group, are implementing a Risk Communication and Community Engagement (RCCE) plan. With the support of over 20 Health Cluster partners, NGOs and INGOs messages have been disseminated across various channels and via social media for the fifth week in a row, reaching tens of thousands of people and vulnerable communities across the OPT.
UNICEF is also taking the lead in coordinating and centralizing the procurement of medical supplies and equipment. Additionally, the World Food Programme (WFP) has set up a logistics working group to support humanitarian partners in providing key supply chains, reducing duplication and increasing cost efficiency. Logistics services will be provided by air and sea, through Ben-Gurion Airport and Ashdod Port.
On 19 April, a senior UN Team met with representatives of the Inter-Ministerial Committee of the de-facto authorities to discuss issues and challenges related to COVID-19. The authorities reaffirmed that the coordination procedures for quarantine facilities remains, that all health requests should be channelled through MoH, and all non-health requests channelled through the Ministry of Social Development (MoSD). Similarly, the UN reconfirmed that WHO will lead the health response, and that OCHA, with the cluster lead agencies, will coordinate all nonhealth related humanitarian assistance to the quarantine facilities. Strong cooperation efforts also continue between the GoP and Israel in response COVID-19.
Needs, responses and constraints by cluster
[For a detailed list of activities by cluster please refer to the annex in the full report]
Health
Needs overview
There is currently no specific treatment for COVID-19. Consequently, the most effective approach to protect the population is containment, with a focus an early testing of all suspected cases, isolation and treatment of confirmed cases, and contact tracing and quarantine arrangements. This must be complemented by primary and communitybased health initiatives, focused on the prevention and promotion of effective protection measures (hand hygiene, physical distancing, etc.). Additionally, efforts must continue to scale up hospital preparedness and treatment capacity to manage an increase in demand for hospital-based patient care.
As part of these priorities, there is an increasing need to mobilize further resources to provide adequate training for all staff working in health facilities, including on clinical case management protocols and infection prevention and control policies. Additionally, local procurement should be emphasised wherever possible, while maintaining quality control. There is a need for a healthcare strategy that maximizes available resources and minimizes the consumption of materials currently in global shortage.
Response overview
The Health Cluster remains committed to reinforcing a comprehensive, multi-sectoral response to the COVID-19 outbreak, while continuing programme delivery and the provision of life-saving assistance. All related activities are directed at supporting the measures taken by the Palestinian authorities, led by the Ministry of Health (MoH).
Interventions have strengthened the MoH’s capacity to early detect and respond to the current COVID-19 outbreak and prevent further transmission of the virus. Mental Health and Psychosocial Support (MHPSS) activities are an integral part of these interventions. Efforts have been also invested in coordinating and streamlining the work of various partners with the authorities.
As knowledge about the virus increases, resources are being re-targeted to support the most effective public health interventions, with an emphasis on the most vulnerable.
Gaps, challenges and constraints
Efforts to address needs related to the quarantine sites have faced various challenges, including a local, regional and global shortage of laboratory supplies for COVID-19 testing, as well as shortages of some essential case management equipment, particularly for critical cases and infection Protection and Control supplies. These shortages are delaying delivery of such items to the OPT, especially in Gaza, and impacting on testing and the COVID19 response. The lockdown of ministries, such as the Ministry of Finance, further complicates the processing of financial procedures like VAT exemption, and the transport of items through borders.
All major providers (MOH, UNRWA, NGOs) have scaled down sexual and reproductive health services as a result of the COVID-19 outbreak, leading to a drop in pregnant women attending facilities, a lack of resources to conduct home/mobile clinic visits and a general shortage of medical supplies, including PPE.
Protection
Needs overview
The need for enhanced mental health and psychosocial support (MHPSS) services has continued to rise. During the reporting period there was a deterioration recorded in this regard attributed to COVID-19 stress factors, including social isolation, health-related fears, and stigma and discrimination. Widespread job losses affecting income and livelihoods are placing significant pressures on families, pushing vulnerable families into further poverty.
Frontline responders (e.g., medical and quarantine staff) are also experiencing increased stress and psychosocial impact. Data from helplines suggests a continued increase in domestic violence against women and children, especially in overcrowded areas. Meanwhile, persons with disabilities or chronic illnesses are facing increasing difficulties in accessing services and information, with some families reporting not having sufficient money to stockpile food and medicine.
In East Jerusalem, Palestinians without Israeli IDs or regularized status are not covered by the Israeli health and social insurances and therefore in need of support to access basic services. Some 160,000 Palestinians living in Shu’fat refugee camp and Kufr ‘Aqab, who are located within the Israeli-declared municipal boundary of Jerusalem, but physically separated from the rest of the city by the Barrier, are also vulnerable regarding access to services. A number of partners operating in East Jerusalem report an increasing demand for GBV and child protection services.
Response overview
During the reporting period, Protection Cluster partners have continued to implement and scale up alternative methods of reaching the most vulnerable population groups, in particular in quarantine sites and remote communities addressing GBV, child protection and MHPSS. Key responses continue to be remote consultations, toll-free helplines and awareness raising campaigns. Implementation of the “Back to Home” project is underway, targeting Gaza quarantine sites to ensure accessibility to MHPSS services and the capacity of frontline staff to detect and refer GBV and child protection cases. The Women’s Peace and Humanitarian Fund has announced a call for proposals under the COVID-19 Emergency Response, to support local women’s organizations.
Gaps, challenges and constraints
Limited access to medical services on the part of isolated refugee communities in Area C and the “Seam Zone”, due to overall COVID-19 restrictions poses significant constraints; this is in addition to the absence of mobile health services and lack of public transportation.
The withdrawal of international protective presence continues to increase Palestinian's exposure and vulnerability to settler violence, which continued throughout the reporting period. Difficulty in ascertaining the impact of COVID19 on children and families. Undertaking an abridged rapid assessment may be necessary.
Education
Needs overview
Following the closure of education facilities in early March, 1.43 million children across the OPT need to access distant learning and receive age appropriate, awareness-raising messages around COVID-19. In isolated and poor areas, 360,000 children without internet connections need home-based learning materials and support. Priority requirements continue to be age-appropriate, awareness-raising messages for children and their families in addition to hygiene-related preventive measures and continuity of learning at home. Some 3,037 schools are in need of cleaning and disinfecting in preparation for the re-opening of schools, as well as an adequate supply of cleaning and disinfecting materials to all schools while they are closed. Latrines in 402 schools need urgent rehabilitation and new clean drinking water points are needed in 134 schools. In addition, an estimated 215,000 children and their caregivers, and 3,000 teachers are in need of psychosocial support through innovative approaches, utilizing social media and phone calls.
Response overview
Education Cluster partners have developed interventions to address the needs set out in the Ministry of Education’s (MoE) Response Plan for COVID-19. Main achievements to date include the mobilization of US$2.5 million for the MoE COVID-19 response plan, which is currently 40 per cent funded and procurement has started of 1,800 cleaning and disinfecting kits for MoE schools. In addition technical and financial support has been provided to over 100,000 children to access various MoE e-learning platforms and remote MHPSS support has been provided to children and their families in coordination with Child Protection partners.
Gaps, challenges and constraints
The scale and nature of this crisis is beyond that anticipated in existing preparedness plans and the capacities of MoE and cluster partners. This includes the lack of platforms for distance learning prior to the emergency, and a lack of consensus between MoE in Ramallah and Gaza over the content of the e-learning platform. This has been compounded by the limited internet connectivity in certain communities and households. The MoE and cluster partners are also not operating at full capacity, due to the movement restrictions and quarantine measures. Finally, there are funding gaps for the rehabilitation of emergency WASH facilities at schools.
Shelter
Needs overview
In the Gaza Strip, people hosted in quarantine centres for the 21 mandatory days need various individual hygiene kits, sterilizing items and non-food items (NFI), such as mattresses, blankets, pillows and mats. Most of these items must be periodically redistributed for incoming people. There are currently 38 facilities identified for potential use as quarantine centres, with a capacity to host up to 5,000 individuals. During the past week around 1,600 individuals crossed through Rafah, bringing the total number of people in 21 quarantine facilities to 2,017.
Additionally, in Gaza, a previous assessment by the Ministry of Public Works and Housing has identified 9,500 dilapidated or substandard homes. The most vulnerable of these households urgently need proper hygienic and disinfection materials, as well as awareness materials concerning hygienic practices and mitigation measures.
In the West Bank, the main concern remains the expected return of Palestinian workers employed in Israel, who require quarantine facilities. The current capacity of identified centres is 5,000 individuals, who will need NFI kits similar to those in Gaza. Also, many requests came to the cluster partners to set-up a pre-screening and registration facilities for the workers at crossings and at the entrances of the Palestinian towns.
An assessment conducted by an NGO of 198 vulnerable communities in Area C found that over half of the residents could not afford the basic hygienic and cleaning materials to combat COVID-19.
Response overview
The Shelter Cluster response seeks to improve the capacity and resilience of vulnerable individuals and households to reduce the spread of the pandemic. In Gaza, partners have continued to aid quarantine centres, with necessary support including NFIs, hygiene and female dignity kits, and cleaning supplies. In the West Bank, 80 tents (originally intended to respond to demolitions) were distributed for use as pre-screening and registration facilities at hospitals, clinics, crossings and town entrances. Across the OPT, around 12,000 hygiene and cleaning materials were distributed to vulnerable families via different institutions and village councils, and educational materials and awareness flyers in coordination with RCCE.
Gaps, challenges and constraints
A main constraint is the lack of quality, household disaggregated information on needs, to accurately target interventions, compounded by the movement restrictions that impede access to the most vulnerable households and communities. The lack of accurate information about the quarantine facilities needs in WB imped the cluster’s ability to mobilize the required NFI materials support.
Water, Sanitation and Hygiene
Needs overview
In coordination with the Palestinian Water Authority (PWA) and service providers, the Cluster is closely monitoring access to WASH services to ensure that the required levels of water and sanitation are not being affected by the COVID-19 outbreak.
As water consumption is increasing in both the West Bank and Gaza, PWA plans to arrange fair water distribution among the communities to satisfy this increase. Meanwhile, there is a continuous need to address the lack of drinking water and hygiene kits in quarantine centres and screening and testing points.
There is an increased demand in monitoring the quality of hygiene materials available in the local markets, as well as the need to raise public awareness regarding the interaction of families with their quarantined family members, and the appropriate hygiene practices to be adopted.
Response overview
During the reporting period, nine WASH cluster partners implemented interventions, reaching around 6,100 individuals. Partners were able to distribute 530 household hygiene kits, and support quarantine centres in Gaza and the West Bank with over 5,000 bottles of water and cleaning materials, eight sets of mobile latrines, along with hygiene and protection materials for health workers.
The PWA has developed its national COVID-19 response plan. The plan includes emergency interventions to ensure the regularity of access to water and sanitation services across the OPT. In Gaza, the main water utility, in coordination with the International Committee of the Red Cross (ICRC) and the Norwegian Refugee Council, supported water service providers with essential sanitization and protection materials. Water service providers have managed to maintain regular levels of supply in the West Bank and Gaza.
Gaps, challenges and constraints
The main challenges identified by the WASH Cluster include:
- Unclear status of some of the quarantine centres in the West Bank;
- Shortage and low quality of hygiene materials on the market, especially locally produced hygiene sanitizer;
- Limited data regarding WASH situation in East Jerusalem neighbourhoods, due to the lack of local specialized entities in the area and the different Israeli COVID-19 monitoring and control systems.
Food Security
Needs overview
The pandemic has already had severe socio-economic consequences, which are expected to increase in the coming weeks, with direct consequences on food security. The Ministry of Social Development (MoSD) estimates that at least 53,000 families across the OPT have fallen into poverty in recent weeks following the loss of a source of income due to COVID-19 restrictions.
Agricultural livelihoods have been particularly impacted. Basic agricultural production is not available at a local level, especially in areas such as agricultural fertilizers, seeds of all kinds, and the most important basic feed for livestock, which are all linked to international trade movement restrictions.
Market transactions are severely limited, as traders and producers cannot physically meet, leading to low demand, limited production, reduced prices and farmers selling at a loss. Dairy production is experiencing a low demand, especially in the northern West Bank. In Gaza, people in quarantine centres rely on external support for their food needs, while farmers, herders and fishers are struggling to acquire agricultural inputs for food production.
Response overview
During the reporting period, partners in the Food Security Sector have continued distributing food parcels to poor families, including through safe home deliveries in the Gaza Strip, and providing hot meals and fresh fruit to persons in quarantine centres. MoSD reported that 28,000 parcels had been distributed so far.
In the West Bank, the MoSD, in partnership with local councils, charitable societies and Zakat committees, has begun tracking and assessing newly poor families, towards a possible distribution of cash and food assistance by the end of April. Across the OPT, the MoSD, in partnership with Food Security Sector partners, has conducted a rapid survey to monitor the availability of food and other basic items on the market.
In the West Bank, the Ministry of Agriculture (MoA) began distributing one million seedlings for home gardens through local NGOs. Additionally, food security partners have engaged in awareness-raising activities about COVID19 and related infection-control practices among farmers and cooperatives. In Gaza, the MoA started the distribution of fodder and fertilizers for farmers and poultry (broilers) breeders, with a total value of US$1 million. 3,000 daily waged workers received cash assistance of US$100 as part of a DFA grant to workers affected by the COVID-19 pandemic.
Gaps, challenges and constraints
In addition to the mobility restrictions affecting all partners, the delivery of cash assistance has been disrupted, as banks have stopped receiving clients face-to-face. Moreover, Cash-for-Work (CfW) interventions are also impacted as many skilled and unskilled jobs come to a halt, although some education and other organizations began implementing a work-at-home modality.
[1] OCHA; the Ministry of Health (MoH); the Palestinian Red Crescent Society (PRCS); and the Union of Health Workers Committees.
subscribe to our mailing list
SUBSCRIBE TO RECEIVE OCHA'S INFORMATION PRODUCTS
OCHA Sites








Follow Us
Support
Your donations go to relief organizations delivering quick and effective support to Palestinians in need.