COVID-19 Emergency Situation Report 1 (as of 1200 hrs, 24 March 2020)
This report is produced by OCHA OPT in collaboration with humanitarian partners. It covers the period from 5 March. The next report will be issued around 31 March.
Highlights
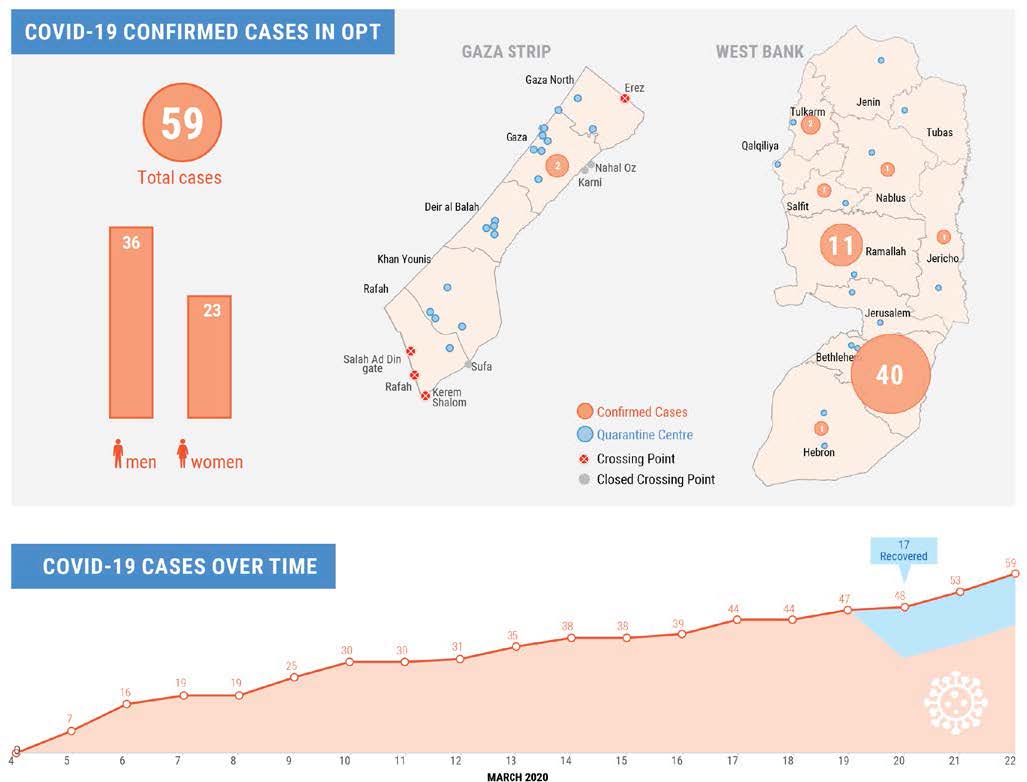
- On 22 March, the Palestinian Authority imposed a curfew in the West Bank for 14 days, obliging people to stay at home, except for the purchase of food and medicine, or in case of emergency.
- First two COVID-19 cases detected in Gaza; 1,400 people held in 21 quarantine centers across the Strip in precarious conditions.
- The COVID-19 Inter-agency Response Plan for the coming three months, is less than 23 per cent funded.
| 59 | 32 | 13,000 | US$6.5 M |
| Confirmed COVID cases | Quarantine centres established | People under quarantine | Initial request for Interagency Response Plan |
Situation Overview
On 5 March 2020, the Palestinian Prime Minister declared a State of Emergency across the occupied Palestinian territory (OPT) in order to contain the spread of COVID-19, after the first cases were confirmed in Bethlehem city. This followed a World Health Organization (WHO) announcement on 30 January of a “public health emergency of international concern”, which was upgraded on 11 March to a “global pandemic”.
As of 23 March, a total of 59 cases have been detected in the OPT, 57 in the West Bank and two in the Gaza Strip. Of the West Bank cases, some 70 per cent are in Bethlehem’s urban area, and nearly 20 percent in the Ramallah governorate (figures exclude confirmed cases in Israeli settlements, which are dealt with by Israel). According to the Palestinian Ministry of Health (MoH), all cases are either asymptomatic or show mild symptoms, and 17 cases have recovered.
West Bank
Incoming travelers from Jordan, as well as people who were exposed to confirmed cases, were initially sent to home quarantine for 14 days, and, from 22 March, to isolation in medical centers in their areas of residence. The number of quarantined people is currently estimated at over 9,900. Confirmed cases of COVID-19 are being referred to two health facilities, in Jericho (the Military Academy) and Turmusayya village in Ramallah (the Hugo Chavez Hospital).
The Palestinian Authority (PA) has been gradually scaling up access restrictions and social isolation measures across the West Bank, including a suspension of all educational activities, a prohibition on public gatherings, a closure of the Bethlehem urban area, and a halt in Palestinian employment in Israeli settlements (the latter measure has been largely unenforced). These measures escalated on 22 March, when the PA announced a comprehensive curfew for 14 days, which obliges people to stay at home, except for the purchase of food and medicine, or in case of emergencies. Public services will be further reduced. As part of the COVID-19 response, the MoH, with UNICEF, WHO and the private sector, activated its risk communication plan, which aims at disseminating public health awareness messages and addressing uncertainty and misinformation.
The Israeli authorities have progressively limited the number of Palestinian workers allowed into Israel. On 22 March, both authorities agreed that Palestinians who intend to keep working in Israel, will be provided with accommodation by their employers and must stay in Israel for at least one month. The Israeli authorities also prohibited the entry of East Jerusalem Palestinians, as well as all residents of Israel, into areas A and B of the West Bank. The access of patients referred to hospitals in East Jerusalem and Israel has been limited to emergency cases and cancer patients. So far, no special restrictions have been placed on East Jerusalem residents, including those who reside beyond the Barrier. The functioning of the commercial crossings with Israel continue without change.
Gaza Strip
Since 15 March, all incoming travelers from Egypt and Israel have been sent to isolation for 14 days to one of 21 compulsory quarantine facilities set up in health facilities or schools, with some 1,400 people currently accommodated there. Additionally, over 2,000 people who entered Gaza prior to 15 March are currently in home quarantine. A field hospital has been established in Rafah to isolate and treat confirmed cases of COVID-19, with the first two cases detected in Gaza on 21 March.
As in the West Bank, all educational institutions have been closed since 6 March. However, other aspects of daily life, including commerce and services, had been less restricted until 22 March, when the de-facto authorities ordered a closure of wedding halls, weekly markets, restaurants and cafes; restrictions were imposed on the holding of public events and Friday prayers.
The Israeli-controlled Erez crossing has been largely shut down since 12 March for most permit holders, including over 5,000 laborers and traders with permits. The exit of patients referred to hospitals in East Jerusalem and Israel has been limited to emergency cases and cancer patients. The functioning of the Kerem Shalom commercial crossing with Israel and the Rafah crossing with Egypt continues without change.
The exit of people from Gaza to Egypt via the Rafah crossing has been halted by the Egyptian authorities as of 15 March; since 23 March, entry of people to Gaza has been suspended. Import of goods via this crossing continues.
Main concerns and priority needs
Although the current number of detected cases remains relatively low, the capacity of the Palestinian health system to cope with an expected increase in COVID-19 cases is severely impaired by longstanding challenges and critical shortages. The situation is particularly severe in the Gaza Strip, where the health system has been undermined by the longstanding Israeli blockade, the internal Palestinian divide, a chronic power deficit and shortages in specialized staff, drugs and equipment.
As elsewhere, the most vulnerable groups, who may require intensive medical, are the elderly and those suffering from hypertension, lung conditions, kidney failure, cardiovascular diseases and diabetes. People living in overcrowded conditions, particularly in refugee camps and densely-populated, poor areas of Gaza and the West Bank, face a higher risk of contagion due to the precarious sanitation systems, including substandard and irregular water supply and shared latrines (more under Shelter Cluster section).
The most urgent items currently in short supply and which are needed to contain the spread of the epidemic and reduce potential mortality among vulnerable groups include: personal protective equipment (PPE) kits and other essential supplies for infection prevention and control; equipment, disposables and drugs for the treatment of respiratory distress; ventilators, cardio-monitors, emergency carts and portable X-Ray machines; and equipment to conduct COVID-19 tests. Hospitals across the OPT have shortages of specialized staff in intensive care units and the laboratory infrastructure urgently requires upgrade to conform with strict biosafety standards, while laboratory staff in Gaza suffer from significant gaps in training and specialized skills. In addition, new stringent national and international travel restrictions pose problems in adequately deploying emergency staff (more under Health Cluster section).
The closure of schools, limitations on access to work places, and the imposition of quarantine and curfew, particularly in overcrowded households, alongside general uncertainty, are expected to increase mental and psychosocial distress, particularly among children, as well gender-based violence. These concerns are particularly magnified in the Gaza context, given the impact of the blockade, three major escalation of hostilities and, most recently, the effect of the high casualty toll from the “Great March of Return”. At the same time, the provision of social services has been severely curtailed due to the access and other restrictions imposed. The implementation of alternative modalities for the delivery of Mental Health and Psychosocial Support Services (MHPSS) to cover the increasing caseload is urgently needed (more under Protection and Education Cluster sections).
The economic impact of the crisis has so far been limited mainly to the workers who have lost their income from jobs in Israel, as well as some businesses in the West Bank, particularly in Bethlehem city, which were forced to shut down. However, in the West Bank, in particular, the volume of people affected by the loss of income is expected to increase soon, following the tightening of restrictions and its impact on all sectors of economic activity (including services, manufacturing, construction and transportation).
In Gaza, the initial macro-economic impact of COVID-19 has been limited. However, the impact of long-term disruptions in Gaza raises serious concerns, given the already-dire economic situation there, with unemployment at almost 43 per cent in the last quarter of 2019, youth unemployment at 64 per cent, and some 53 per cent of the population living below the US$4.6 poverty line (more under Food Security Sector section).
Inter-agency response plan and humanitarian operations
Under the direction of the UN Resident and Humanitarian Coordinator (HC/RC), UN agencies and NGOs have developed and begun implementing a range of interventions to support the Palestinian authorities’ efforts.
At the heart of these interventions is the Health Cluster COVID-19 Interagency Response Plan. The Plan details initial priority actions, critical over the next three months, to address immediate shortages and capacity gaps in the health system, while enhancing preparedness efforts by the MoH for a worst-case scenario. This initial plan aims to stop further transmission of the virus; to provide adequate care for affected patients and support to their families; and to mitigate the impact of the epidemic (including through MHPSS). The Plan also includes a communications component, involving the dissemination of health advice, to mobilize the community and combat rumors and misinformation (For more about specific activities see Health and Protection Cluster sections below).
The plan in its current form seeks to mobilize for US$ 6.5 million to support these efforts. The funding requirement across sectors is likely to increase significantly due to the scale of the pandemic and the progressive expansion of the response to critical elements of different sectors.
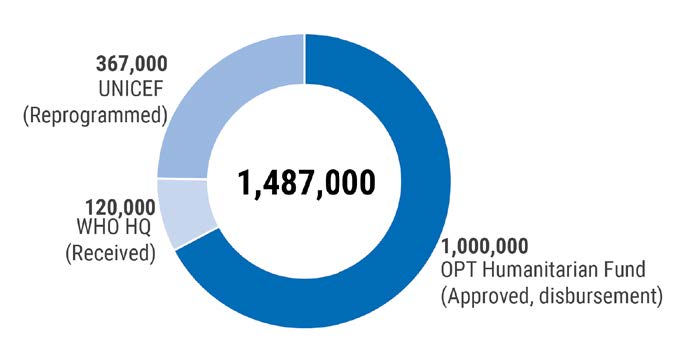
Of the total appeal, less than $1.5 million has been raised so far, including $1 million allocated from the OPT Humanitarian Fund, $120,000 by WHO corporate funds and $367,000 reallocated from UNICEF’s budget (see also Funding matrix at the bottom of the report).
Activities covered by the plan are supplemented by additional interventions addressing other aspects of the crisis and carried out by partners in the areas of food security, shelter and non-food items, protection, education and water, sanitation and hygiene (WASH) (more in the Cluster response sections).
Additionally, UNRWA has launched a separate Flash Appeal, seeking $14 million to cover COVID-19 related interventions across its five areas of operation (Lebanon, Jordan, Syria, Gaza and West Bank), also for the coming 90 days. Proposed activities include preparedness and response measures at UNRWA health and education facilities, and coverage of health expenditures for vulnerable populations.
Humanitarian partners are making efforts to maintain critical components of regular programmes and health partners continue to scale up responses. In addition, food distribution, protection, WASH and responses to both demolition and settler violence incidents continue. Due to tightened access restrictions, humanitarian partners have had to prioritized urgent humanitarian interventions only.
Following the initial release of the Health Cluster plan, partners are working across the board to identify broader support requirements and update the initial plan, which should be launched in the days, while the Palestinian authorities develop their own integrated plan for response.
Coordination
Since the start of the crisis, the Palestinian and Israel authorities have maintained a close, unprecedented cooperation on efforts aimed at containing the epidemic. Representatives from both ministries of health, as well as from Israel’s Coordinator for Government Activities in the Territories (COGAT) have been meeting on a regular basis to agree on matters of mutual concern, such the understandings concerning Palestinian workers employed in Israel. As part of these efforts, COGAT is facilitating four trainings for Palestinian medical teams, while the Israeli MoH donated over 1,000 testing kits and thousands of PPEs to the West Bank and Gaza. Despite longstanding tensions and disputes, there has been also continuous cooperation and coordination between the Ramallah-based Palestinian Authority and the Gaza-based Hamas authorities, around efforts to address the current crisis.
Under the auspices of the HC/RC, an inter-agency Covid-19 Task Force has been established which meets several times a week, to set policies and coordinate the response. The HC/RC is also convening a weekly general coordination meeting with a wider group of partners and an information meeting with donors.
The HC/RC and OCHA are also engaging on a regular basis with relevant Palestinian authorities, including the Prime Minister’s Office and Palestinian Civil Defense; and with Israeli authorities, including the COGAT and the National Emergency Management Agency (NEMA).
The Inter-Cluster Coordination Groups (ICCG), in both the West Bank and Gaza, are responsible for coordinating the implementation of the Task Team decisions and monitoring the impact of movement restrictions on regular humanitarian programming.
The HC/RC also informs the Palestinian authorities about essential movements required by humanitarian and development staff during this period of enhanced movement restrictions. Where necessary, coordination with the Israeli authorities is also conducted for safe movement in the West Bank. A Standard Operations Procedures (SOP) has been developed to guide agencies in identifying and submitting requests for essential staff movements.
Funding for COVID-19 interventions
Funding Received for the Health Cluster Interagency 90-day Plan
|
Donor |
Amount |
Status |
Recipient |
|
OPT Humanitarian Fund |
$1,000,000 |
Approved disbursement |
WHO & Partners |
|
WHO HQ |
$120,000 |
Approved, disbursement |
WHO |
|
UNICEF |
$367,000 |
Reprogrammed |
UNICEF |
|
Total |
$1,487,000 |
|
|
Funding Pledges Received to Support Response to the COVID-19 Outbreak in OPT
|
Donor |
Amount |
Status |
Recipient |
|
World Bank |
$ 800,000 |
Received |
MOH |
|
World Bank |
$ 50,000,000 |
Pledged |
PA |
|
Austria |
EUR 250,000 |
Pledged |
|
|
Qatar |
$ 10,000,000 |
Pledged |
|
|
Kuwait |
$ 5,000,000 |
Pledged |
WHO |
|
Qatar |
150,000,000 |
Pledged |
TBC |
|
DFID |
|
Expressed interest |
UNICEF |
|
Canada |
|
Expressed interest |
UNICEF |
|
SDC |
|
Expressed interest |
UNICEF |
Concerns, priority needs and responses by cluster
Health and Nutrition
Concerns and priority needs
Based on the current epidemiological situation in the eastern Mediterranean region, the risk to OPT is considered very high. Additional risk factors include high prevalence of non-communicable diseases and smoking amongst the population; large number of vulnerable people, including refugees; a fragile public health system, particularly in the Gaza Strip. Priority needs, primarily in Gaza, include the following:
- Personal protective equipment (PPE) kits and other essential materials and supplies for infection prevention and control, such as fumigators and disinfectants. Literature shows that a significant proportion of medical staff are at risk of contamination, and if health workers are infected, this has a knock-on impact for the entire health response. In the Gaza Strip, only 700 PPEs are currently available.
- Additional supplies for COVID-19 testing for proper surveillance and containment. To date, the Gaza Strip only has 1,000 swabs and 500 tests.
- In Gaza, vital laboratory supplies and upgrades of infrastructure are needed to conform with strict biosafety standards. Training for laboratory staff is also mandatory.
- Supplies for case management at health-designated facilities for COVID-19 patients, particularly oxygen concentrators; ventilation packs for critical care; and supplies for patients classified as severe, but not in intensive care units (ICU). Support for the Rafah Field Hospital, which is receiving confirmed cases, and the European Hospital in Gaza is critical.
- Upscaling ICU and acute care personnel, in addition to training existing health workers, including primary healthcare staff, paramedics, emergency department staff and intensive care nurses and doctors.
- Addressing additional non-COVID-19 caseload in Gaza, which includes some 1,700 patients referred to East Jerusalem hospitals, who were prevented from travelling due to the closure of the Erez crossing, along with some 4,000 additional elective surgeries postponed, due to preparedness measures (in addition to over 8,000 pre-existing cases).
- In the next three months, there will be over 30,000 births in the OPT. Due to increasing pressure on the health system and restrictions on movement, it is important to avoid disruptions to life-saving services for women and newborns, including antenatal care, postnatal care, and family planning services.
Response
As part of the Health Cluster plan, partners have carried out the following activities:
- Procured and distributed to MoH facilities 2,500 PPEs, including surgical masks, medical masks, gowns, gloves and goggles, as well as other medical supplies and hygiene products. By the end of March, 60,000 protective gowns and 13,000 surgical masks will be delivered.
- UNICEF is supporting nine implementing partners in Gaza and six in the West Bank through the procurement of essential hygiene supplies. Some US$ 18,000 worth of infection prevention control (IPC) items are to be shipped to key implementing partners to support the delivery of maternal and child health and nutrition, and early childhood development services.
- CARE International is supporting the Palestinian Medical Relief Services, a frontline care provider, with PPE and IPC supplies.
- An assessment of the sexual and reproductive health (SRH) needs, in light of COVID-19, is ongoing to best inform response. UNFPA is providing PPE for partners delivering SRH services.
- WHO and Cluster partners are supporting the MoH in assessing and preparing isolation and quarantine units and providing guidance for proper case management.
- WHO will procure additional testing kits and laboratory supplies, support the MoH to expand laboratory capacity, including rehabilitating the central public health laboratory, and conduct training workshops for laboratory detection.
- WHO will support the MoH to enhance existing respiratory disease surveillance systems, as well as establish active case findings at points-of-entry, health facilities and within communities. The case-definition for COVID-19 has been expanded to include all severe acute respiratory infections to increase case detection.
- The Risk Communications and Community Engagement taskforce delivered posters and brochures to the MoH and health partners and supported the scaling up of MoH’s public awareness campaign through SMS, TV and radio. WHO’s introductory online course on COVID-19 was made available in Arabic.
- UNICEF is supporting the introduction of hotlines for the promotion of appropriate nutrition among pregnant, lactating women and infants and young children, along with COVID-19 prevention counselling. The hotline services will be operated in Gaza and West Bank by two NGOs.
Protection
Concerns and priority needs
The protection sector’s capacity has been negatively impacted by the access restrictions and other measures. For example, out of UNICEF’s 18 child protection partners, 5 have completely halted activities and 12 have seriously curtailed them. Partners are unable to operate until safeguarding protocols and hygiene materials are in place, and many households do not allow access to home visits due to heightened fears of contagion. Meanwhile protection concerns for the vulnerable population have increased:
- Fears about the virus, economic stress and quarantine measures increase household tensions. This exacerbates women and children’s vulnerabilities and puts them at increased risk of various forms of violence, including intimate partner violence, gender-based violence and sexual exploitation and abuse.
- In the Gaza Strip there is a chronic lack of safe places and recreational areas for children. Over 500,000 children now spend their days at home, with many playing or working in the streets. The disruptions and related mental health stressors increase risks to children, such as anxiety, trauma, psychosocial relapse and increased violence.
- The poor living conditions at the quarantine centers in the Gaza Strip including lack of privacy and adequate WASH facilities.
- The withdrawal of international protective presence actors in the West Bank has increased the exposure and vulnerability of some communities to settler violence. A key protective presence NGO (EAPPI) estimates that the suspension of its five teams will affect over 200 communities.
- 150 vulnerable children (14 to 17-years-old) are impacted because of the closure of vocational training centers. The Ministry of Social Development (MoSD) in the West Bank reported that all female Child Protection Counsellors are working from home, and there are limited response capacities in place.
- The crisis has also curtailed access to support services for GBV survivors creating a significant response gap with movement restrictions and reduction in or suspension of services. The MoSD shelter for women in Bethlehem is no longer accepting new cases, and the girls’ shelter in Beit Jala is also operating in emergency mode.
- Legal aid providers have suspended activities involving in-person interaction, including ‘walk in clients’ for counselling and paralegal services, conducting group information and training sessions, advocacy tours, and representing cases in courts. In the West Bank, despite the postponement of hearing sessions by the Civil Administration, inspectors continue to distribute demolition orders.
Response
The Protection Cluster is closely monitoring emerging vulnerabilities, protection and human rights issues, while supporting mitigation measures to address the implications of COVID-19 on protection work including:
- Steps to re-orient work and mitigate and address gaps with alternative methods of service delivery. Child protection and MHPSS partners have initiated alternatives such as mobile appointments, free telephone counselling, virtual learning, distributing awareness leaflets and requesting movement authorization in emergency cases. GBV service providers have offered remote consultations, organized social media and radio campaigns, and expanded toll-free Helpline services.
- An emergency team of 27 responders has been set up in the Bethlehem area by local NGOs in partnership with the Union of Social Workers and Psychologists to provide psychosocial support for individuals who are affected by COVID-19 and in isolation and, more broadly, to respond to the population’s needs.
- An emergency plan for sheltering services is being developed by the NGO-run shelter in Gaza, in case a woman asks for shelter, while a general quarantine is imposed in the Gaza Strip. The Hayat Center will coordinate with the MOH to conduct blood count testing where there is a concern. Women with respiratory illness symptoms may stay at the dedicated room for GBV survivors at the Shifa Hospital in Gaza City.
- As replacement activities for GBV services, UNFPA has encouraged virtual and social media outreach, radio spots and phone counselling. Some partners have developed social media and radio campaigns to address increasing stress on women and risk of GBV.
- The GBV Sub-Cluster has shared information materials with all partners for further dissemination and sent 500 hygiene and dignity kits to quarantine facilities in Gaza.
Shelter and Non-Food Items (NFI)
Concerns and priority needs
Considering the general advice to maintain social distancing and avoid gatherings to reduce the spread of COVID19, the Shelter Cluster’s main concern is the overcrowded living conditions that exist in the Gaza Strip, particularly in refugee camps. Interventions to reduce overcrowding are urgently needed to mitigate the exposure and risks among vulnerable populations.
- An estimated 5,000 households in Gaza that do not meet minimum shelter standards need support to improve those standards, particularly regarding overcrowding. Measures include the increase of covered living spaces, alongside further household partitions. The estimated cost is $2,000 per household. • Another 2,000 households in Gaza rely on common latrines and other facilities, which generate a health hazard. Affected families require additional sanitation facilities. The estimated cost is $1,000 per household.
- Additionally, some 20,000 individuals in quarantine facilities and vulnerable households, in both Gaza and the West Bank, need non-food and hygiene items kits, along with awareness materials, at a cost of $70 per kit.
Response
Shelter partners are providing assistance to the quarantine centres that have been established for incoming travelers in Gaza. On 17 and 18 March, agencies distributed over 4,000 non-food items (mattresses, blankets, pillows, mats), some 500 hygiene kits and 250 tarpaulin sheets to 10 PA schools in Gaza, which have been set up as quarantine facilities.
Education
Concerns and priority needs
All education facilities across the OPT have been closed since 6 March. These include 3,037 schools, of which, 2,300 are in the West Bank and 737 are in Gaza, along with 2,017 kindergartens (KG). A total of 1,430,000 children are affected as a result, 57 per cent in the West Bank and 43 per cent in Gaza. Principal emerging needs include:
- The provision of distance learning: the Ministry of Education (MoE) requires e-learning materials and platforms to ensure continuity of learning from home.
- An estimated 360,000 children across the OPT living in households without internet connection need hard copy, home-based learning materials.
- All 1.43 million affected children need to receive age-appropriate information about COVID-19.
- 5,000 schools and KGs need systematic cleaning and disinfecting in preparation for the re-opening of schools.
- 215,000 children and their caregivers, and 3,000 teachers, need psychosocial support via social media and phone calls.
- Latrines in 402 schools in Gaza and the West Bank need urgent rehabilitation and another 134 schools require new clean, drinking water points.
Response
The Education Cluster has supported the development of a MoE Response Plan, and embedded the Education Cluster Coordinator in the Ministry of Education. The plan was finalized and disseminated among stakeholders on 17 March. Four task teams have been established to support the implementation of: distance learning; provision of MHPSS; promotion of hygiene and renovation of WASH facilities at schools; and distribution of school hygiene kits. The task teams will contribute technical capacity and the financial means to implement the plan. Main steps implemented included:
- Starting procurement processes for some 15 per cent of hygiene and cleaning kits to schools;
- Cluster partners beginning engagement with the MoE on content and IT solutions for distance learning;
- Coordinating with Protection Cluster partners the provision of remote MHPSS to children and their families; and Key Cluster partners beginning mapping funds that can be re-allocated to the response plan.
Water, Sanitation and Hygiene (WASH)
Concerns and priority needs
The main concern is to ensure continuous access to safe drinking water and sanitation, despite increasing restrictions, to minimize the impact of COVID-19. Current needs identified by the Palestinian Water Authority (PWA) and other service providers, to ensure cleaning and disinfection of WASH facilities include: the procurement of calcium hypochlorite and other sterilization materials, for an initial cost of approximately $188,000, and the rehabilitation of key WASH facilities.
Response
While a detailed WASH response plan is under elaboration, cluster partners have undertaken the following:
- Support to the Health Cluster plan through hygiene promotion and adaptation of ongoing WASH interventions to respond to the current emergency.
- Activation of the WASH Cluster Contingency Plan and the prepositioning of spare parts, tanks and hygiene kits to respond to the emergency.
- UNICEF have supported the MoE providing hygiene kits to 200 schools, 80 in the West Bank and 120 in Gaza.
- Rehabilitation works of WASH facilities in seven primary health care clinics and three family centers.
- Improvement of the water network at Al Shifa Hospital in Gaza, as well as provision of sanitizers and mattresses covers for two critical departments.
Food Security
Concerns and priority needs
At this stage, the Food Security Sector has not identified a significant increase in needs. Nevertheless, food insecurity could be deepened in the context of the pandemic, both in terms of the quantity of people being affected, and the severity of food insecurity. Food insecurity in the OPT is already high, particularly in Gaza Strip (62 per cent). The main drivers are poverty, unemployment, and reduced resilience. Decreased availability of food poses an additional potential risk. This may be caused over time by a) disruption of local value chains, which could determine market spikes of local produce, and b) disruption of regional or global value chains that could void the capacity of import to keep local prices low. The following are additional compounding factors:
- Delivery of UNRWA and the World Food Program (WFP) in-kind and e-voucher food assistance to over 1.2 million people in the Gaza Strip might be disrupted, should curfew be imposed there. As of 22 March, the first round of UNRWA food distribution covering Q1-2020 is yet to be completed, with around 60,000 households still approaching UNRWA food distribution centres (DCs) for receipt of food baskets.
- UNRWA’s closure of all schools and some programmes providing community services led to the suspension of some Cash-for-Work opportunities.
- Palestinians in the West Bank employed in Israel and Israeli settlements constitute 17.7 per cent of the labour force. If these workers become unemployed, food insecurity in the West Bank will increase, and new vulnerable groups will emerge.
- Food security responses to demolitions in the West Bank, including assessments and deliveries, will be stopped.
Response
- WFP and UNRWA have advanced the start of their joint food distribution programme to herding communities in the West Bank, from 1 April to 16 March (i.e. currently ongoing), in anticipation of curfew measures.
- To avoid overcrowding, UNRWA expanded the number of food distribution centres, adding 12 facilities (schools). Non-refugees assisted by WFP can be supported until June through food e-vouchers.
- UNRWA has also reassigned part of the Cash-for-Work beneficiaries employed in the education sector to other positions needed for COVID-19 preparation (e.g. security guards, cleaners, labourers).
The current epidemic is not a typical shock to the food system and requires rapid adaptation to a new operating environment in both the short and medium term. In order for the food security sector to adapt to the new way of working, interventions should target farmers and fishermen, workers in the agri-food industry and the most vulnerable food consumers. Support packages to be considered in the short-term include: ensuring safe access for farmers and fishermen; provision of essential production inputs; supporting the MoA to adapt and continue delivering critical services; and supporting the MoSD to provide direct food access and cash assistance to the newly unemployed.
subscribe to our mailing list
SUBSCRIBE TO RECEIVE OCHA'S INFORMATION PRODUCTS
OCHA Sites








Follow Us
Support
Your donations go to relief organizations delivering quick and effective support to Palestinians in need.