
Agencies urgently require $21 million to respond to casualties in the Gaza strip
Since 30 March 2018, Palestinian casualties in the Gaza Strip have increased significantly due to the mass demonstrations taking place along the perimeter fence with Israel and, to a lesser extent, hostilities and other incidents.
To respond to this crisis, humanitarian agencies have prioritized three areas of intervention: emergency healthcare; protection monitoring; and mental health and psychosocial support (MHPSS). The total funding required for these interventions from 30 March until the end of 2018 is US$43.8 million, of which $22.7 million has been contributed to date, leaving a shortfall of $21.1 million.[1]
Of the 28 projects in the proposed response, 11 are part of the broader 2018 oPt Humanitarian Response Plan (HRP). However, the HRP for the oPt is one of the most poorly funded in the world and is only 29 per cent funded at present. [2]
The shortfall exacerbates already overburdened institutional service delivery systems and threatens the continuity of minimum operational capacities in Gaza.
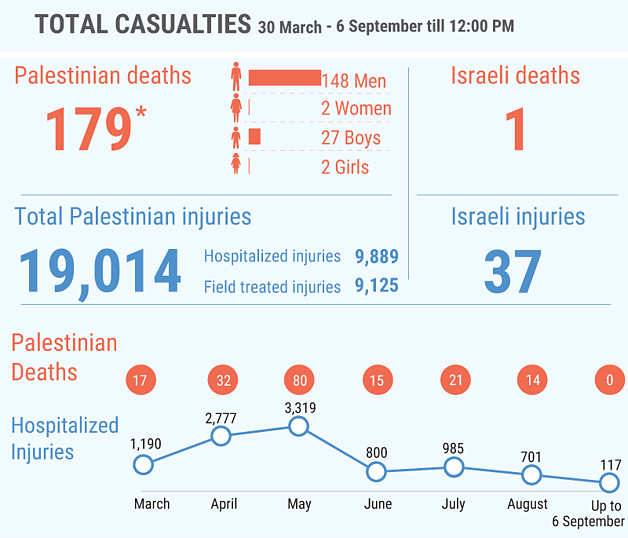
From the start of the ‘Great March of Return’ demonstrations on 30 March up to the end of August, a total of 179 Palestinians, including 29 children, have been killed by Israeli forces: 130 during the demonstrations and 49 in other circumstances; over 18,700 others have been injured, including 1,642 children. [3] One Israeli soldier was killed by Palestinians and another 37 Israelis were injured.
Around 52 per cent of the Palestinians injured required hospitalization. The large number of casualties among unarmed demonstrators who did not pose an imminent threat of life or deadly injury to Israeli soldiers, including a high percentage of demonstrators hit by live ammunition, has raised concerns about the excessive use of force.
 The current surge in humanitarian needs takes place against a backdrop of an already precarious humanitarian situation in the Gaza Strip; the health system is on the verge of collapse and there is widespread despair as conditions deteriorate and hope for a sustainable solution fades.[4] Gaza’s health sector is collapsing in the wake of the now 11-year blockade, the deepening intra-Palestinian political divide, the energy crisis, inconsistent and reduced payment of public sector staff, and growing shortages in medicines and disposables.
The current surge in humanitarian needs takes place against a backdrop of an already precarious humanitarian situation in the Gaza Strip; the health system is on the verge of collapse and there is widespread despair as conditions deteriorate and hope for a sustainable solution fades.[4] Gaza’s health sector is collapsing in the wake of the now 11-year blockade, the deepening intra-Palestinian political divide, the energy crisis, inconsistent and reduced payment of public sector staff, and growing shortages in medicines and disposables.
Emergency healthcare
Emergency trauma management is most important during the first hours in which an injury is sustained. During demonstrations health providers and humanitarian partners have deployed to field locations to provide first aid and reduce the need for hospitalization. Acute inpatient surgical care at the hospital level is essential to avoid loss of life and prevent disabilities. This includes complex reconstructive wound and orthopaedic care, complex pediatric and adult anaesthesia, intensive care, blood transfusion and rehabilitation services.
 in the field. © Photo Credit: WHO")
Public hospitals in Gaza currently have extremely limited capacity to manage complex inpatient surgical care or post-operative rehabilitation. Dealing with a high caseload of trauma patients is beyond the capacity of even advanced and fully equipped hospitals. In Gaza, where the health sector is already suffering from electricity cuts and severe shortages of drugs, medical supplies and staffing, hospitals are unequipped to handle such a caseload. As a result, by 27 August, 270 patients injured in demonstrations had been referred for medical treatment in the West Bank, Israel or Jordan, and had applied for exit permits via the Erez Crossing: only 63 applications (23 per cent) were approved and the remaining were either denied (37 per cent) or are pending (40 per cent). [5]
Rehabilitation and post-operative care is limited, leading to increased infections and further potential complications. A recent analysis by the Health Cluster estimated that by the end of 2018, over 1,200 patients with limb injuries would require complex and timely limb reconstructive surgery; these are highly complex injuries that, if not treated, may heighten the risk of secondary amputations. From 30 March until 6 August, there were 72 amputations: 14 of them on children and one female patient. Of this total, 64 were lower limb amputations and eight were upper limb amputations. To manage the influx of trauma patients, the trauma pathway across pre-hospital, hospital and post-hospital and rehabilitative care services in Gaza urgently needs to be scaled up.
Non-trauma patients suffer because treatment and healthcare for urgent medical conditions is interrupted as the wider health system responds to the casualties from the demonstrations. Some 8,000 pre-scheduled surgeries (some of them critical cases for which a delay can affect prognosis) have been postponed. In June, the waiting time for elective surgery at the largest hospital in Gaza (Shifa) was 64 weeks, well beyond the Ministry of Health (MoH) threshold of 24 weeks.[6] Delays to surgical interventions may prolong suffering and ill-health, and may have a negative impact on the psychological and social life of the patient. In some cases, delays can lead to further medical complications.
Until end August, health partners had received approximately $21.5 million in new funding for trauma management and emergency healthcare. This has enabled a range of critical interventions to be introduced, including the deployment of 14 international emergency medical teams; some 21,000 outpatient consultations; more than 9,000 post-operative wound management consultations; provision of assistive devices to over 6,600 patients; and the delivery of 15,600 lifesaving drug items and 315 disposable items. The World Health Organization (WHO) has established the Gaza Trauma Working Group to ensure a coordinated and quality emergency response from the point of injury to rehabilitation. Additionally, on 9 August, the International Committee of the Red Cross (ICRC) opened a temporary post-operative ward in a pre-existing building at Shifa Hospital, which includes 20 beds. To continue covering needs across the trauma pathway until the end of 2018, health sector partners require an additional $20 million.
Protection monitoring
During the first weeks of protests at the perimeter fence in Gaza, the high number of casualties and violations gave rise to the need to expand monitoring, data collection, verification and reporting, alongside timely analysis, to inform the humanitarian response. The capacities of protection partners to monitor events effectively as the casualty figures grew were clearly limited, not least due to pre-existing funding gaps.
Of particular concern, health personnel and facilities have been exposed to violence. Up to 27 August, three health staff have been killed, 404 injured, 59 ambulances and five other health vehicles damaged, and two health facilities damaged, reportedly by Israeli gunfire.[7] Attacks on health staff and damage to health facilities and assets are not only detrimental to staffing and facilities, but also to patients requiring emergency health services.
Additional capacity is particularly required for documentation and monitoring of child casualties and any encouragement given to children to engage in protests that pose potential harm. As Israel/State of Palestine is a “Situation of Concern” on the agenda of the Security Council, protection partners are required to submit inputs to the annual report of the Secretary-General on Children and Armed Conflict. As such, independent sources are required for the emergency monitoring of incidents of Children and Armed Conflict (CAAC) or grave violations of children’s rights.
Up to end August, responding partners in the Protection Cluster had received some $284,000. This has funded the recruitment of 10 additional field workers to verify and document possible violations; to provide analysis for other programmatic responses; the enhancement of coordination mechanisms; legal counselling to 137 individuals; and legal aid, including one petition to the Israeli High Court of Justice on behalf of individuals requiring travel permits for urgent treatment outside Gaza. Partners require an additional $476,000 to scale-up and maintain these responses until the end of 2018.
Mental health and psychosocial support (MHPSS)
WHO projections of mental disorders in populations affected by emergencies show that up to five per cent of the population may display a severe mental disorder in the 12 months following an emergency. A further 20 percent may display a mild or moderate mental disorder. As a result of the current crisis in Gaza, it is estimated that approximately 10,400 people will have severe mental health problems and 41,700 will have mild to moderate problems requiring MHPSS, including 26,000 children. These numbers are expected to increase as mental health incidents tend to be manifested at a later stage after the events.
Prior to the recent events at the perimeter fence, demand for services already exceeded existing institutional service delivery capacities due to chronic underfunding and the government salary crisis. In late 2017, the Child Protection Working Group (CPWG) of the Protection Cluster estimated that over 295,000 children needed structured psychosocial support and child protection services, with at least 11,000 children in Gaza estimated to require case management in 2018.[8]
As part of the emergency preparedness mechanism in Gaza, Governorate Protection Focal Points have been visiting injured children to assess their situation and provide psychological first aid (PFA), although they have not received funding and staff have not been paid since March 2018. Following these primary field assessments, children are referred for case management and psychosocial support services. Existing funding allows family centres to operate at a minimal capacity but they cannot meet an increase in demand. Significant resources are required to expand outreach and the response of family centres to provide critical services. The reality is that unless under-resourced child protection services are invested in, children in need will be at significant risk of developing serious mental health issues.
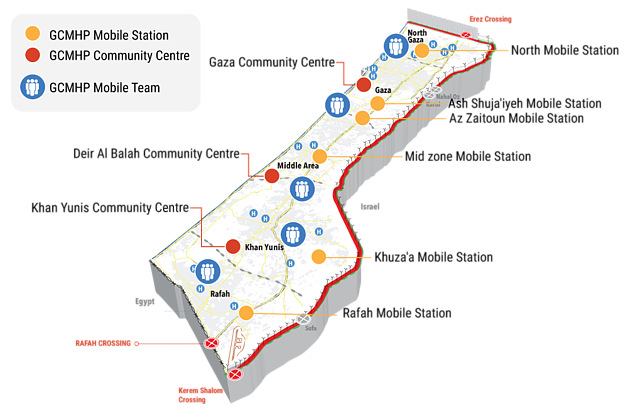
By end August, three MHPSS partners had received $967,000 through the oPt Humanitarian Fund. This funded 10 mental health professionals to provide PFA to 4,000 adults and 500 children through hospital and home visits; counselling and specialized therapeutic mental health services to 400 people at six mobile stations established for this purpose across the Gaza Strip, combined with free telephone counselling to 300 people; and raised community awareness of the psychological and social impact of trauma on the Gaza Strip population, the risk of engaging in protests and information on available services. To scale-up and maintain these responses until the end of 2018, partners in the MHPSS sector require an additional $660,000.
Emergency fuel about to run out
Lifesaving services in the Gaza Strip are currently dependent on the delivery of UN-procured emergency fuel, mainly to power back-up generators that operate during Gaza’s daily power outages. Gaza’s energy crisis leaves its two million Palestinian residents, over half of whom are children, with only four to five hours of electricity from the grid per day. A sum of $4.5 million is urgently needed to ensure sufficient supplies of emergency fuel to power essential services until the end of 2018. If funding is not secured immediately, the emergency fuel will run out completely in September. Gaza’s most vulnerable people, who rely on public services and have limited income sources, will be the hardest hit.
Key services in the 14 public hospitals such as elective surgery, sterilization and diagnostic services continue at reduced capacity. More than 4,800 patients daily in Gaza require access to lifesaving or life-sustaining healthcare with a constant supply of electricity. At least 300 of these patients are connected to lifesaving medical equipment such as ventilators, dialysis machines, incubators and anaesthetic equipment. Any disruption or electricity cut puts patients at immediate risk of brain damage or death. There is also an increased risk of waterborne disease across the Gaza Strip if supplies of emergency fuel are not renewed.
Gaza Community Mental Health Program (GCMPH) centres, mobile stations and PFA mobile teams
Services to people with cerebral palsy disrupted following Israeli air strike
On 14 July, following an escalation between Israel and Palestinian armed groups in the Gaza Strip, the Israeli air force targeted and partially destroyed a building in Gaza City which, according to the Israeli military, was used by a Palestinian armed group for “militant training and exercises”. Two 14-year-old children who were sitting on the roof of the building at the time of the attack were killed and another 31 people, including five children, were injured.
Several adjacent buildings were also damaged as a result of the airstrike, including the “Palestine Avenir for Childhood Foundation” (PACF), an institution that provides specialized rehabilitation services for around 3,000 children and adults suffering from cerebral palsy,[9] including physiotherapy, occupational therapy and speech therapy. The PACF centre also accommodates a primary school for 140 children from first to third grade and a kindergarten (16 classrooms in total), and helps with adult learning and the reintegration of children with disabilities into mainstream education.

As the PACF building was empty at the time, the airstrike did not result in casualties but there was considerable damage to doors, windows, ceilings, rehabilitation equipment and furniture with costs estimated at $180,000. Most services had to be halted except for a few activities that continued in the less damaged rooms. Subsequently, PACF resumed services at alternative temporary locations until repairs to the damaged building are completed.
Since July 2018, PACF has extended its response to community outreach and assessment of the needs of more than 120 demonstrators injured in demonstrations. It also provides multi-disciplinary services, including medical and PSS support, and rehabilitation.
The Israeli attack that damaged the PACF premises has raised concerns about international humanitarian law (IHL) provisions relevant to the conduct of hostilities. Under IHL, as a rule, only combatants and military objectives can be targeted; any military attack, even when directed at a legitimate military target, must comply with the IHL requirements of necessity, precaution and proportionality.
[1] The initial appeal was launched on April 2018 for a period of two months but has been updated twice since then to reflect the increased needs up to the end of the year due to the demonstrations continuing beyond the initial timeframe and the outbreak of limited hostilities.
[2] Figures as on 16 August 2018, Financial Tracking Service.
[3] The source for injury figures is the Palestinian MoH in Gaza. For further details on casualties see OCHA oPt snapshot.
[4] Please refer to the 2018 Humanitarian Needs Overview and 2018-2020 Humanitarian Response Strategy documents for a detailed analysis. Both documents can be downloaded from the OCHA oPt webpage.
[5] WHO Situation Report, available here.
[6] Source: WHO monthly monitoring system.
[7] WHO Situation Report, available here
[8] Based on analysis conducted by the CPWG for the 2018 HNO.
[9] Cerebral palsy is a group of permanent movement disorders that appear in early childhood.
SUBSCRIBE TO RECEIVE OCHA'S INFORMATION PRODUCTS
OCHA Sites








Follow Us
Support
Your donations go to relief organizations delivering quick and effective support to Palestinians in need.